
Amidst a global push for mass vaccination as the battle against COVID-19 rages on many people are still afraid to be vaccinated.
People remain concerned about the perceived ‘experimental’ nature of vaccines, whether they should be worried about short term risks such as blood clotting and myocarditis; and long term risks including side effects relating to DNA changes, fertility and reproduction, and other unknown long term chronic illnesses and side effects further down the track.
A lot of people continue to wonder whether the risks of vaccination outweigh the benefits.
Greek City Times spoke to trained scientist and medical professional Dr. Nicholas Lelos in our search for answers to some of the questions currently circulating around the controversial topic of vaccination, and here is what he had to say.

Preface by Dr. Lelos
The science is constantly changing and there are multiple new sources of information. I think the most important thing to establish is that people need to be wary of sources, as there is a lot of anecdotal evidence and misinformation.
The most rife one, unfortunately, is that provided by several individuals that are prefaced by Dr. – when this could be a PhD of certain institutions, a higher degree into a non-medical specialty (such as a nutritionist), or from institutions that have lax criteria in awarding the title. These individuals go on and publish their opinions and “evidence” that they highly cherry-pick on their own website, or some other sites of little to no accreditation or peer-reviewing, whereupon they then reference and draw whatever conclusions they wish.
Even a fully trained medical doctor, however, is not immune to various influences, and of having an agenda.
This is particularly evident in the United States, where a lot of authoritative narratives come with sponsoring from either competing pharma companies, anti-vaxxer sites or organisations, or even religious bodies that are trying to alter the narrative.
My personal advice, as a trained scientist before doing medicine – just because it is published, available online, or even appears in a Journal, do not ever take anything as established fact: the key skill here is critical appraisal. This involves finding many different sources, checking their credentials and biases/conflicts of interests, then assessing the quality and level of evidence they furnish.
Critical appraisal is a difficult and lengthy task – and a lot of people have confirmation bias, where if they see something that vaguely echoes their existing beliefs or ideas they are most likely to jump on it and not question it. It is important to look at patterns and identify various factors that can impact the question studied.
My own personal declaration is that I have no vested interests in the writing of this article, I receive no money or endorsement from institutions or of big pharma.
I only offer my experience and knowledge as someone who is a front-line clinician, and I am at the very forefront of the pandemic since the very beginning – a protected population is everyone’s priority, from my patients to my friends and family.
Let us move with the questions.
Are there treatment alternatives to vaccination?
Some have suggested that safe and effective early treatment alternatives exist such as hydroxychloroquine and ivermectin in place of vaccination. Is it true that the “refusal of health authorities to issue early treatment guidance has contributed to the mortality rate of the disease?”
To paraphrase another colleague – there is a difference for clinical care involving individual patients, where you can see a lot of horrible side effects and consequences, and public health or epidemiology, which is the study of entire populations.
Public health is about finding solutions for multiple populations, whilst also looking into environmental impacts on health, genetics, historical cultural effects and even governmental.
The individual effect of a single drug can do miracles for an individual, or even 10 or 100, or your relatives, or even work well for one doctor or a group of doctors using it at a specific location with certain groups of patients – this will not, however, mean that it will work across the entire population. And this is what the policy is made of, and what the World Health Organisation (WHO) are basing their decisions from.
The refusal of these health authorities basically entailed not using their population as test subjects for medications that have never been tested for this purpose. It would have been acceptable in Victorian times but there was also a really high accepted death risk which most people may struggle with nowadays.
So to answer your question – there is currently no evidence that these medications work in severe or life threatening COVID.
Dexamethasone, a steroid, works when patients are gravely ill and about to be mechanically ventilated – this has been studied, reduces mortality and ventilation needs.
Supplements and vitamins boost the immune system, so they help generally in health- but they do not treat COVID. And you need to have deficiencies of vitamins to benefit from supplementation anyway.
Hydroxychloroquine is a hideously potent medication used for malaria and immunosuppression, and has a relatively narrow window for it to do its effects before becoming toxic. A single tablet can kill children below 6 years of age. Definitely not a good option to have lying around the household. Here is a summary of the current state of these so-called remedies https://www.bmj.com/content/370/bmj.m3379
Here is an excellent live article that is getting constantly updated as new information gets out with other treatments for COVID and the evidence https://www.bmj.com/content/370/bmj.m2980
Why the push for global vaccination in place of such alternative treatments?
If it is true that there are safe and effective early treatment alternatives such as hydroxychloroquine and ivermectin, why the push for global vaccination?
So as stated above there are no other effective early treatment alternatives. Even steroids that work for severe COVID, when studied for mild cases, did not have a benefit.
Vaccinations, on the other hand, have worked time and time again – small pox and polio have been eradicated, and measles was almost controlled – until the rise of vaccination hesitancy when people did not have the stark reminders of their children dying on them or having life-long disabilities (such as with polio).
Global vaccination has worked in the past.
What is herd immunity and how does it relate to the COVID vaccine?
Herd immunity is a principle where a certain amount of the population needs to be immune in order for the disease to not be able to spread. As it requires hosts to go and infect more people, if enough people have immunity then the disease can not make the jump to infect new hosts – and thus protect even people with no immunity, such as the newborn, the immunocompromised or people who develop allergies to the vaccine.
The problem that has come up with this pandemic, is that the different strains of the virus, and individuals immune systems, can elicit a different response in people – studies have shown that even getting the virus and having a small course of illness means that you do not generate enough antibodies to protect yourself for long.
Meaning that you can get re-infected, or hit with a different strain.
The concept of vaccination is that it causes a sufficiently strong immune reaction that not only stays for longer but is also more effective against multiple strains. So just getting COVID may not protect someone enough, compared to getting a vaccination or boosters.
This is an approach that has been used very effectively for hepatitis B as well.

‘Experimental’ Vaccine
The vaccine has been referred to as ‘experimental’ is this true and should we be concerned?
The technology has actually been around for 40 years. So I would hardly call it new.
Experimental would be accurate in the sense that the vaccines that we use did not have a large period of time to be tested, compared to other medications or treatments – but this is usually how any medication or treatment made its debut.
Usually wars and pandemics lead to rapid progress of medical sciences because there is more of a drive to not let people die. Penicillin started in a similar fashion – and it is one of our most effective and life saving medications. One of my friends was actually in the Oxford drug trials – now she is fully protected.
I have to say, the difference though in this scenario and the past is stark - big pharma drug and medication research and development, because of our extremely tight regulatory environment, used to take a long time to assess for safety, but also a lot of the data was not made public. So that the companies could make money.
Now, entire countries are being exposed, but the data is transparent and available to all, an extraordinary achievement in the sense that they are not allowed now to sweep mishaps or issues under the carpet anymore.
Also, external agents and scientists are able to look at the effectiveness data and how well vaccines work without interference from the parent company.
Vaccination and the Issue of Informed Consent
In the push for vaccination the government mentions ‘informed consent.’ Informed consent must be given prior to administration of the vaccine. Is this a way for the government to avoid responsibility for any future side effects down the track considering that there is not enough data for anyone to ascertain long term effects on the body of vaccination?
Informed consent is one of the linchpins of medical practice – you need to let people know about ALL the possible side effects before administering a treatment or procedure, no matter how exceedingly rare they can be. This has always been the case, and is not new.
We have been using vaccination as a principle for nearly 100 years – the side-effects of getting COVID, on the other hand, are pretty immediate and quite dramatic.
Which groups should not be vaccinated? (For example - those who have recovered from COVID-19 and many groups have no possibility of benefiting from the vaccine, including younger individuals, pregnant women, women of childbearing potential, and those with immunodeficiencies) and why?
So as for who should get it, this is where we are still learning – Israel has managed to vaccinate its entire adult population and will be proceeding to reduce the age to include children – so more information will be available.
So the very young will probably not be vaccinated at this point, the elderly definitely, emphatically should, as they are the population with the highest complications.
Pregnancy and being of childbearing potential has not shown any impacts at this stage. The numbers that we have for clots are extremely small from the vaccines – whereas pregnancy and cancer, or even COVID, increases your risk several orders of magnitude up.
Immunodeficiencies such as HIV or immunocompromised patients due to organ transplants or renal dialysis, however, are still at the forefront of research – because they do not seem to generate the immune response that the vaccine requires to provide protection. There is a recent initiative to see whether 3 doses are required for these patients. More information coming soon!
Vaccination and the Issue of ‘Gene Therapy’
What do you think about claims that the global push towards vaccination is a strategy aimed at securing emergency use authorization (EUA) for COVID gene therapies? Why are some people referring to the vaccines as COVID gene therapies? Is this what they are?
I believe this is the usual rhetoric to ‘trigger’ people, such as GMO food – it does not mean what people think.
Gene therapy has a very specific goal – replacing the patients’ genes, who are usually having defects causing diseases such as cystic fibrosis, with the gene sequences that aims to correct the areas that cause the diseases. Or to enhance the gene structure to provide protection against diseases, such as the recent case with the scientist in China who was aiming for producing resistance to HIV. All of them rely on being able to affect directly the patients’ DNA structure.
To date, this approach has not been successful – the closest we have come is to identify what is missing from the body (proteins) and to provide them to the patient.
These vaccines are definitely not gene therapies – they do not affect the DNA.
They work by providing mRNA, which is the blueprints that our cells in our body use to make proteins – we are using it ourselves for our own proteins. So vaccinating provides our body with the ability to produce, from ourselves, a component of the virus, which on its own can not infect you.
This is in contrast with previous vaccines, such as the tetanus one, which used to give chopped components of the organisms, or of the live attenuated vaccines, which use the actual virus but weaken it so it does not have the strength to infect the host.
Those have been used extensively over the decades, but have inherently more risk for allergic reactions, or of reactivation.
This mRNA delivery is far more elegant, and far more efficient in providing to the body what it needs to mount an efficient immune response without putting it at risk of getting the infection in the first place.
How the COVID-19 Vaccine Works in the Body
What is mean by a “toxin spike protein factory”? Do you think that this what is happening to the bodies of those being vaccinated? Do the vaccines ‘coat our DNA’ or ‘change our DNA?
So this is complete balderdash – the mRNA from the vaccines would need to penetrate the core of our cells, and be transcribed into our DNA – which is impossible on its own without several other components.
mRNA is what comes from the DNA being “read” in order to synthesize proteins. Once it is read, it produces the spike proteins that are coating the outside of the virus – it is what it needs to “hook” into our cells and infect them.
So it is both a key component of the virus, and hence important for our immune system to recognise quickly and efficiently, but also quite useless on its own – it is like having a key without a hand behind it to insert it into the lock.
This is what the spike protein factory refers to – our own cells have protein factories, this is how our DNA is used – we are just borrowing our manufacturing ability to give us copies of these keys to prime our own immune system.
HIV, on the other hand, has got a reverse transcriptase that integrates it into our own DNA – which is why no vaccines have been able to be made for it all these years.
Vaccine Side Effects and Long Term Health Effects
Do the COVID vaccines "trick the body into making the spike protein of the virus?” Is it true that the vaccine is distributed in an uncontrolled way throughout the body and can potentially affect different organs of the individuals depending on where their body makes the spike protein? Could this potentially effect the reproductive organs?
I would like to highlight something interesting here – the words used. “Tricked”. There is no tricking – the body gets given blueprints to make the same components as the virus to identify it and use it for a better immune response before getting infected.
It is the virus’ way into the hosts cell – it is not, by itself, causing the disease. Otherwise everyone who got a vaccine would be getting COVID. And this is the problem that we highlighted earlier – the single case by case scenario can be different between patients or a group of patients, but when we are talking about populations you look at the big picture.
The disease control centre in the US is currently reviewing evidence about whether the vaccine is causing neurological conditions, such as Guillain-Barre Syndrome. My last reading of the data was about 100 cases reported in 12.5 million vaccines. The average background rates in the US are 10 in 1 million of population, because this condition is usually caused by viral infections.
The direct consequences of COVID are much, much higher and can cause direct neurological damage – because you don’t just get the spike protein but the whole package.
https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2779759
No correlation has been found so far with the reproductive organs, and pregnant women have been vaccinated without any different effects to the ones that are not pregnant.
This is really important, as the initial trials did not include pregnant or lactating women – so this is real world data with about 30000 vaccinated pregnant women that were studied and are being followed up.
Should we be worried about other long term health effects of being vaccinated?
It is only sensible to worry about the unknown or new treatments that have not been around for long enough – on the other hand COVID poses a very real and documented risk both for short term and long term consequences.
Long COVID has been found to be quite devastating as it affects the heart, the lungs as well as possibly the brain.
Should we be Worried about DNA Changes, Cancer and Chronic Illness as Possible Side Effects?
Of course we should be worried, and of course big pharmaceutical companies pumping the entire population full of substances that are potentially harmful should make us cautious.
All our cells have a place in how they operate – reverse transcription would indeed make it possible to get components integrated into our DNA. There are cells that need to do partially such operations, like the cells of our immune system – in order to store the memory of this information so it can recall it when the body gets infected with COVID.
For the entire DNA of every single cell of our body to be changed, or at least the stem cells or germ cells that turn into sperm and eggs, to cause a permanent DNA mutation, would involve a level of technology or exposure of something that currently is only present in science fiction movies.
As highlighted before, this would be gene therapy. And the argument is vacuous – the body generates the spike proteins. The virus also has these proteins.
So whether you are getting them from the vaccine or the virus – the vaccine does not cause the infective consequences of the virus. These proteins can not be incorporated into the DNA.
Also any cell that has a deviation from the original program gets identified and destroyed by the body anyway – this is the whole reason why we do not have more cancer or immune diseases.
Should we be concerned about our children being vaccinated and damaging long term effects on their health or for example reproduction or passing on DNA changes to babies?
For the reason mentioned above, as the vaccine has no ability to affect the germ cells, the answer is currently no.
But everyone is exerting the highest amount of caution before wanting to try it with children – the current variants up until now seem to not cause them much distress – but reports have been coming of some new strains that have been infectious and cause injury to younger age groups too… Watch this space!

Vaccine Ingredients
Should we be concerned about the vaccine ingredients? Some theories include that the ingredients include fetal cells – can you please explain this further and should we be concerned about this?
No concerns about the vaccine ingredients – now more than ever. Even the minute concentrations of metals that were used in vaccines decades ago have all been switched to inactive inert substances (see table I below).
| Description | Pfizer-BioNTech (mRNA) | Moderna (mRNA) | Janssen (viral vector) |
| Active ingredient | Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 | Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 | Recombinant, replication-incompetent Ad26 vector, encoding a stabilized variant of the SARS-CoV-2 Spike (S) protein |
| Inactive ingredients | 2[(polyethylene glycol (PEG))-2000]-N,N-ditetradecylacetamide | PEG2000-DMG: 1,2-dimyristoyl-rac-glycerol, methoxypolyethylene glycol | Polysorbate-80 |
| 1,2-distearoyl-sn-glycero-3-phosphocholine | 1,2-distearoyl-sn-glycero-3-phosphocholine | 2-hydroxypropyl-β-cyclodextrin | |
| Cholesterol | Cholesterol | Citric acid monohydrate | |
| (4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2-hexyldecanoate) | SM-102: heptadecan-9-yl 8-((2-hydroxyethyl) (6-oxo-6-(undecyloxy) hexyl) amino) octanoate | Trisodium citrate dihydrate | |
| Sodium chloride | Tromethamine | Sodium chloride | |
| Monobasic potassium phosphate | Tromethamine hydrochloride | Ethanol | |
| Potassium chloride | Acetic acid | ||
| Dibasic sodium phosphate dihydrate | Sodium acetate | ||
| Sucrose | Sucrose |
Fetal cell lines have been used since the 1960’s to trial many of our established treatments and vaccines in the past such as rabies and hepatitis A – no parts of the cells or the DNA is in the vaccine, but they have been used to trial whether they worked or not. They were not used to produce the vaccines.
The fetal cell line usage, incidentally, has even been accepted by the Catholic church as able to be used for the common good and re-ratified in 2017. The benefits from these cells have saved millions of lives.
Does the Oxford/AstraZeneca vaccine contain animal/ chimpanzee DNA?
No this is patently false.
It uses an adenovirus (common cold virus) that has its ability to replicate snipped and replaced with the instructions for our body on how to make the spike proteins. So similar outcome to Pfizer or Moderna, but by using a carrier instead.
There have been videos circulating showing metal such as spoons and coins sticking to the injection site on the arm as if magnetised. Why is this happening? Do the vaccines contain any ingredients that would cause this? Is this cause for concern?
Unfortunately, as someone who is working in the front lines as an essential worker, therefore receiving both shots as a priority, and surrounded by colleagues, I have to report that neither myself nor any of my thousand colleagues that I worked with have developed super powers or magnetic abilities.
I would love to see such feats in person.
Effectiveness Against Different Mutations and Over Time
Why are some people still vulnerable to the virus even after vaccination?
Because the vaccination does not make you immune – it does however decrease your risk of dying or being hospitalised from it by 100%.
The problem is when you have only received one shot and your immunity is not fully primed – or immunocompromised.
The current scientific theory is about a partially vaccinated person with HIV being the source of one of the current strains in the UK as the virus has more chances to evolve in a partially protected individual and get more ways to infect us.
And people on dialysis or with solid organ transplants are always at risk because of the immune system deficiencies they have or acquire.
Once vaccinated are people protected against the many mutations of the virus? Or will they need to keep getting booster vaccinations to keep up to date as the virus continues to mutate?
Currently it looks like the vaccines are providing robust protection for the mutations we have circulating – the problem is in vaccine hesitancy.
The more people that are not vaccinated, the more chances the virus has to produce new strains or trying out ways to evade our defences – even those provided by the vaccines.
The current scenario is that it will probably need to happen annually – same as the flu shot.
A third shot has been advocated really recently by Pfizer – this has to be taken with a grain of salt as clearly this will have financial implications for the company, and they stand to make more money if this was enforced.
At the moment it looks like immunity is holding for people having received 2 shots, and a third is not indicated unless if it is considered for immunocompromised individuals.
Does the vaccination provide lifetime immunity? How long does the vaccination stay in the body for? Do you need to have a booster further down the track or are you protected for life?
No it doesn’t, the vaccination does not stay in your body for very long at all but the antibodies that are generated by the body to protect itself seem to be holding so far.
This is clearly been looked at even as we speak to see how long it is effective for. So far 12 months seem to have gone by and it is still effective.
A booster shot looks likely in an annual or bi annual fashion.

Safety and Mechanisms for Risk Mitigation
In comparison with the usual safety measures in place for other vaccines, what safety measures are in place for the COVID vaccines?
Same as with any medication or treatment that is been released into actual clinical use – reporting of adverse incidents on points of care.
Either GPs, hospitals or even individuals themselves. Emergency departments are very aware of possible complications and we are usually the first point of call of anything that is out of the ordinary.
The Australian College of Emergency Medicine has even made a robust guideline for anyone presenting with symptoms after the JJ or AZ vaccine:
The National Health Service in the UK or Australia do not have issues with reporting and collecting that data, or seeing people immediately with suspected side effects and treating them immediately for free.
This is again a very unique situation – the approach to the vaccines transcends national boundaries and has had multinational input, with several governmental and non-governmental bodies monitoring the scene constantly.
This has been unprecedented and is very reassuring. Also the CDC (Centres of Disease Control and Prevention) of each country is scrutinising these results and recommending safety measures within each country.
Which Vaccine?
What are the risks associated with each type of vaccine that we should be aware of? For example the FDA (US Food and Drug Administration) has issued warnings for myocarditis with Pfizer and Moderna and cavernous venous thrombosis with Johnson & Johnson, certain vaccines are associated with children and young adults developing myocarditis, inflammation of the heart. Where can people go to access such data relating to the safety of the vaccines? And statistics relating to risk?
I have provided a table that summarises most of these – created by YourLocalEpidemiologist who is an expert in the field and has been monitoring the pandemic since March last year, and keeping on top of the science as well.
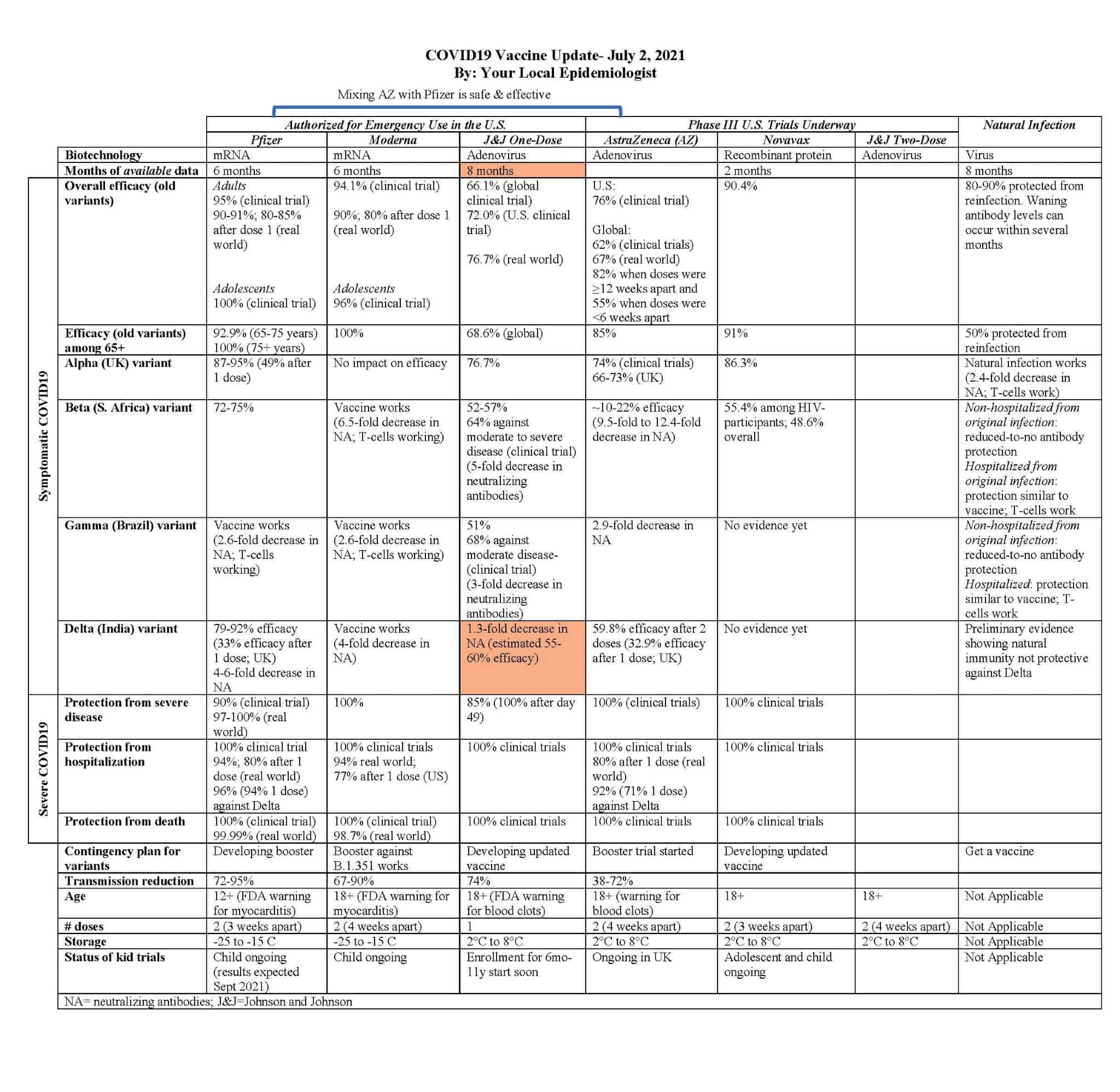
There are risks, as with any medications – unfortunately all that can be said for certainty at this point is that the risks of COVID far exceed that of the vaccines at this point.
And getting infected does not magically give herd immunity, as some immune responses were not sufficient to provide lasting immunity – and then you get reinfected. Which also increases the risk of the strain mutating and becoming more virulent. This is part of the problem of not just letting the disease run its course.
Pros and Cons
Looking at the statistics cited relating to side effects of the COVID vaccines compared with risk of being infected by the disease being cited by some as 1% chance, do you think that the benefits of being vaccinated outweigh the risks?
The problem with statistics is you can make them dance and show whatever you want them to show.
Of course on a population level, 1% does not sound much – that is 1 in 100 young people. Would you want to be that 1 person, when 2 jabs from a vaccine could have prevented it?
And across the population of a country such as Australia, for example, healthy adults below 50 is not the entire population – what about the unhealthy below 50s and the above 50s? The chance of being infected by the disease for these risk groups is much higher than 1%.
Anyone who uses “never” “always” and “ever” when it comes to science has to be approached with caution. Such dogmatism, for something that has not been experienced in this scale for a 100 years since 1918, is unbecoming of a scientific mindset.
Accepting that vaccinations are the only solution, of course, is also not scientific – we have to acknowledge that new information becomes available all the time, and be willing to reassess with new information.
Currently, the state of the science indicates that vaccines are effective, and reduce serious or life-threatening COVID. It is as simple as that – and hence I got vaccinated myself.
So yes, the benefits outweigh the risks.
Best Sources of Information
How much do our GPs know about the vaccines? Are they realistically able to give reliable advice about whether or not to be vaccinated when there is no long-term data available? Or about which vaccine is the safest to take? Where is the best source for those seeking further information about each vaccine and which one is the best for them to take?
GPs are dependent on their own research as the governments unfortunately have not been consistent – the UK government has had a particular bad approach; the Australian government and the media have completely focused on the negative aspects and gave an ambivalent picture, which has led to vaccine hesitancy and as a result, the current Sydney lockdown is a direct correlate from that.
At this precise moment, any vaccine is better than no vaccine, particularly if there is COVID cases nearby. AZ is not going to be continued in Australia, but the immune response across Pfizer and AZ seem to be compatible even if you had one shot of one and then a different shot. There are new vaccines that are coming out, see the table provided.

I would not advocate for any vaccine specifically at this point, but it appears that the Pfizer and Moderna have had the least reported side effects.
I would also like to highlight that many of the perceived side effects of the vaccinations can also occur without them and also by COVID itself. In fact the risk of clots with COVID is 1 in 5 versus 1 in 1 million, even with AZ.
People seem to be afraid to make a decision about being vaccinated as there is a lack of information about the best sources of unbiased information. What do you think are the best unbiased sources to help people become more educated about the vaccines?
There are several sources of data, the only problem is that raw data can be quite lengthy and confusing and requires scientific training.
Then if you choose to go to other experts to provide you with the condensed information, be wary about agendas and ulterior motives of whatever view they are advocating - including vested interests in pharmaceutical companies, of course (of which I have none).
The WHO and the CDC have got good sources, and are generally helpful.
Scientific publications such as Nature and Science can be quite approachable, whereas medical journals are more difficult to absorb and there has been noted to have occasional bias present.
If in doubt approach your local medical practitioner and have a chat, or ask for more information.
The only way we can get out of the current situation is for a surge in vaccinations and for herd immunity to protect our vulnerable members of society.
Data relating to the number of people who have experienced adverse side effects versus data showing the effectiveness in the fight against the virus of being vaccinated
The information in this article is not intended to be provided in place of the advice of your own medical professional. Please seek the advice of your own medical professional before making any decisions with regards to your health.

ABOUT Dr. Nicholas J Lelos
Twitter @DrLelos
LinkedIn: Nicholas Jason Lelos
Medium: doctorlelos
Dr Nicholas Jason Lelos is an American-born doctor of Greek descent, currently residing in Australia, Darwin.
Completing all of his schooling in the French system, Dr. Lelos initially trained as a neuroscientist at the University of Edinburgh in Scotland, and a recipient of a prestigious NATO Fellowship from the Greek government for his work in neuroendocrinology.
Having secured a NHS bursary, he proceeded to study and complete a medicine degree at St George University of London, one of the leading medical establishments of the UK.
He continued to work in London as an internal medicine doctor, with his final rotations being at the world-renowned cancer hospital, the Royal Marsden, having also worked rotations in surgery and general practice.
Dr. Lelos was also a trade union representative with the British Medical Association and was a national representative both as a medical student as well as a junior doctor to the Representative body of the organisation.
The next logical step from the experience gathered in this role was to apply and becoming a Medical Practitioner Tribunal Service Panellist with the General Medical Association, the regulatory body of medical practitioners in the UK, both as a Fitness to Practice as well as an Interim Order Panellist, having to adjudicate and determine medicolegal matters pertaining medical practice of peers.
Being a lover of education and learning, he was engaged at running problem-based learning tutorials and being an examiner for his medical school as well as doing a post-graduate degree in Medical Education with University College of London and the Royal College of Physicians.
He also worked as a Viral Challenge Physician in a research capacity for a company called Retroviral, which specialised in the inoculation of quarantined volunteers with the prospect of running tight, rigorous and scientifically sound clinical trials of medications and treatments for viral infections for universities, research groups or private companies.
Having moved over to Australia, he continues to teach at University of Notre Dame, shaping the medical minds of the future, whilst also retraining in Emergency Medicine in South Western Sydney, namely Bankstown, Liverpool and Royal Prince Alfred Hospitals, before moving for a stint to the Canberra Hospital and now currently based at the Royal Darwin Hospital in the Northern Territory.
Representing his peers, he was elected New South Wales representative for his trainee peers in Emergency Medicine, before being chosen as the Trainee Representative Chair for the College of Emergency Medicine until the end of 2019, a role which he pursued vigorously having to travel across Australia and interact with multiple Emergency doctors and departments.
He is still involved in the College, working on reformulating the curriculum and providing better educational material for training.
